Contraction and Labour - Mother's e-Guide

Main menu:
Antenatal

Pregnancy as Childbirth Begins: The First Stage of Labour
Labour is signalled through contraction. Basically, while the foetus develops, the wall of the uterus stretches forward but when the baby is ready to be born, the operations of the uterus is absolutely in the reverse order. The uterus stretches inward against the baby. It is the pressure that is known as contraction. Apart from contraction, the onset of labour could also be signalled through the discharge of mucus stained with blood. This often precedes or goes along with the painful contraction and within 24 hours of its appearance, all things being equal, labour will commence.
In the same vein, uterine contraction usually forces the rupture of the membrane which forms the amniotic sac. Its resultant effect is that there will be a flow of fluid through the birth canal thereby points to the commencement of labour. The breaking of the sac normally speed up the starting of labour. As a result, labour always start within few hours of spontaneous breakage of the sac. In some cases where labour refuses to start within 12 to 24 hours despite the breaking of the sac most especially when pregnancy is close to full term, “Oxytocin” is administered to speed up its commencement.

True Labour versus False Labour
In the last week of pregnancy, the uterus will be increasingly sensitive with more painless contractions and sometimes could be painful. Painful contractions often times occur at night at irregular intervals - this is a false labour. Yes! This is due to the irregularity in duration and mode of occurrence; and with time the contraction reduces in intensity and eventually disappears. Research has affirmed that false labour occurs at night; while its effect is felt at the back and lower abdomen.
On the other hand, in true labour there is an increasing frequency and intensity in contraction at predictable regular intervals. Initially, contraction of true labour lasts about 30 seconds occurring at regular intervals of about 15 minutes to 20 minutes. This can be accompanied by mild pain; the pain increases at some point and later reduces to vanish completely. With the progression of labour, contraction will extend from 30 seconds to 90 seconds while intervals in between contraction usually drop from 20 minutes to 5 minutes. All the while, intensity of contraction will continue to increase and later becomes more frequent such as coming at about every 5 minutes to 10 minutes. At this point, the pregnant mother is advised to visit the hospital.
At the first stage of labour, the muscles of the uterus are in constant contraction so as to stretch and widen the cervix for the baby to pass through into the birth canal. This is known as “Cervical Dilatation” and once it is achieved, the first stage of labour comes to an end. Often times, it lasts for about 10 hours. At this very period, it is expected of the pregnant woman to be relaxed: she can be reading, chatting, listening to the radio or watching the TV etc.
Appropriate widening of the cervix (detected via pelvic examination) is aided not only by uterine contraction but also with the use of the mother’s abdominal muscles as she pushes down hard. Contractions at this stage are strong with cramps, backache and pelvic pain which could be severe. The level of the expectant mother’s preparation for labour will significantly help her to cope at this period and throughout the labour process. However, the Obstetrician may use local anaesthetic injection on the expectant mother to ease the pain while episiotomy may also be conducted to safeguard the pregnant woman from perineal tears or tissue tear in the vaginal opening. It is worthy of mentioning that the urge to push out the baby will be present at this first stage of labour but this is not encouraged as the cervix is not yet fully expanded.
Second Stage of Labour
The beginning of this stage is often revealed through the breaking of the amniotic sac which leads to the gushing of fluid from the vaginal. Usually, it occurs at the end of first stage of labour and at times not until the baby is ready to be born but it is not a rigid phenomenon hence rupture may occur much earlier. The second stage of labour is shorter than the first lasting less than one and half hours. It is the period when the mother-to-be has work to do by using her abdominal muscles to push the baby through the birth canal for delivery. The urge to push is constant at this point due to the pressure of the baby’s head on the tissues in the middle of the pelvis.



Summarily, with each uterine contraction coupled with the to-be mother’s pushing effort, the baby’s head moves closer to the opening between the labia majora (pudendal cleft) and with a continuous push, the baby’s head becomes more visible to the Doctor who then holds gently the baby’s head in his hand. Gradually, still with the aid of further contraction and pushing of the baby further downward, the head sweeps more over the vulval tissues: forehead, eyes, nose, mouth and chin appear in a successive order as the whole body slithers out. Hooray! A baby is born.


Third Stage of Labour: The Last Bit – Afterbirth.
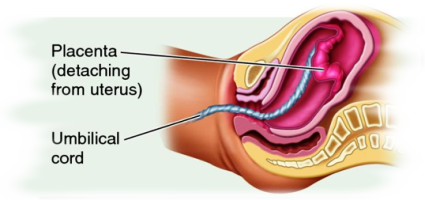
A successful child birth is commendable but the new-born is still attached to the umbilical cord and placenta after delivery; its separation is highly important for both the mother and the new-born to be free. Therefore, the delivery of the ‘afterbirth’ marks the third stage of labour. It usually takes between 5 to 20 minutes or more.
The expulsion of the ‘afterbirth’ occurs either naturally or induced. Once a baby is delivered, the mother will experience a mild contraction; in which naturally, the uterus will continue to contrast and shrink in size. As a result, the tissues of the placenta are forced to split off from the uterine wall. The mother with few pushes will then get rid of it through the birth canal. Sometimes, the doctor can also help in the rapid delivery of the ‘afterbirth’ by pressing down on the woman’s abdomen (top of the uterus) while she pushes simultaneously at the right time.
‘Medical-induced’ ejection is another option; practised using either Picotin (Oxytosin), Ergometrine or Syntometrine injection. They boost uterine contraction for speedy expulsion of the ‘afterbirth’. The injection is given as the head of the baby shows up in the vulval cleft or immediately after the shoulder appears. The injection also helps in the shrinking of the uterus back to normal size while bleeding is reduced. The shrinking of the uterus back to its size is called INVOLUTION, a process that takes about six to eight weeks.
** Afterbirth consists: the amniotic sac, umbilical cord and the placenta.
Home Page | Antenatal | Postnatal | Neonatal | Healthy Tips | FAQ | Trainers Pack | Extras | General Site Map